What kinds of anesthesia are available for children having eye surgery?
There are two main types of anesthesia: local and general. Local anesthesia consists of numbing the area around the site to be operated on by applying or injecting anesthetic agents. For example, dentists use local anesthesia by injecting lidocaine in the area of the tooth to be operated on. The patient is still awake, able to move and is aware of the procedure. General anesthesia puts the whole body to sleep and greatly reduces/eliminates the possibility of movement during the procedure. The patient is not aware of the procedure and does not have any pain during the procedure.
Children will almost always need general anesthesia in order to have any surgery in or around their eyes. This is necessary so that the child is completely still and the surgery can be done safely and effectively. General anesthesia is sometimes needed for a complete examination of a child who is extremely uncooperative to the point that the ophthalmologist cannot obtain crucial information in the office.
Minor eyelid procedures may be done under local anesthesia, but this requires the patient to be still and cooperative.
How is anesthesia administered to children?
General anesthesia is usually given to children in two stages. First, a relaxing drug is given which causes the child to drift off to sleep. This drug is usually delivered as a gas through a scented face mask. An intravenous (IV) line is usually placed in a vein of the arm or leg after a young child is asleep from the mask. Older children may have the IV line placed before going to sleep.
In short procedures, such as opening a blocked tear duct, sometimes only a mask is needed to deliver the anesthesia and complete the procedure. For most eye procedures, however, a breathing-tube or laryngeal mask airway (a special type of tube that may cause less irritation and decrease sore throat after surgery) is placed in the windpipe to allow the anesthesiologist to control and support the child’s breathing while under anesthesia. Inhaled anesthetic agents delivered through the tube and/or medications given intravenously maintain the anesthesia. The breathing tube is removed at the end of surgery before the child is fully awake. The IV can be removed in the recovery period when the child is drinking well and has no nausea. Figure 2 is a photo of an endotracheal tube.

How is anesthetic “sleep” different from normal sleep?
Anesthetic “sleep” is quite different from normal sleep because the potent medications affect every organ of the body. Achieving and maintaining the desired effect requires continuous monitoring and adjustment. Your anesthesiologist has the experience and knowledge to decide which agents are best for your child and to administer them in a safe manner.
How should you prepare a child for surgery?
If your child is old enough to understand why he or she is having the surgery, it is important to provide an explanation so that they are comfortable with the decision. If the child is very young, then being calm and cheerful for them is helpful. Your hospital may provide services such as Child Life to help with this process by playing with and talking to the child before the surgery. If you have any questions please ask any member of the hospital team. The staff, nurses, and doctors will try to make the hospital experience a positive one.
Is a medical examination needed for children before undergoing general anesthesia?
Yes. Before surgery a medical history and physical examination is performed to be sure your child is sufficiently healthy to undergo anesthesia and to have any planned surgery. This will likely be done by the child’s primary care physician and the anesthesiologist as well as the ophthalmologist.
Do anesthesia complications tend to run in families?
Yes, there are certain reactions to anesthesia that run in families, as well as hereditary medical conditions that can make administering anesthesia more complex. Be sure to speak with your child’s anesthesiologist regarding any known adverse reactions to anesthesia that have occurred in your child’s blood relatives. These complications can be severe such as malignant hyperthermia or less severe, but still uncomfortable, like nausea and vomiting. There are steps that can be taken and/or medications which can be given to help with these potential complications.
What can a child eat or drink prior to general anesthesia?
Patients undergoing general anesthesia should not eat or drink anything for a certain amount of time before a surgery is performed. This period of time may be 4-8 hours, depending on the age of the patient and the type of food or liquid. The specific requirements for your child will be given to you directly by the hospital.
Having a completely empty stomach helps avoid pulmonary aspiration. Pulmonary aspiration occurs when stomach contents are breathed into the lungs and can cause serious complications. Fasting can be difficult for anyone, especially children, but please remember it is done for the child’s safety.
The hospital staff will give you specific instructions about what time your child must stop eating and drinking. Please follow them exactly as advised to avoid delay or cancellation of the procedure.
Can a sedative be given to calm a child before going into surgery?
Depending on the surgery your child is having, this may be done. Many hospitals will give a liquid sedative to children prior to surgery to help ease any apprehension. A sedative comforts children as they await their surgery, reduces anxiety as they move into the operating room, and helps them forget the events immediately associated with their surgery.
Isn’t general anesthesia dangerous

Patients are extensively monitored by the anesthesiologist while they are asleep. Serious reactions to anesthesia are extremely rare. All precautions are taken to ensure the child’s safety while he or she is asleep.
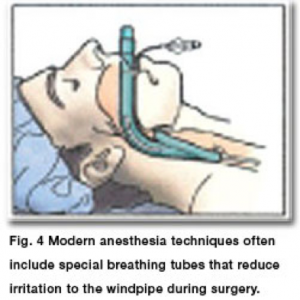
What is a laryngeal mask airway?
A laryngeal mask airway (or LMA) is a special breathing tube which is positioned on top of the vocal cords instead of going past them as an endotracheal tube does. This may reduce irritation to the windpipe during surgery and lessen sore throats afterward [See figure 4]. LMAs are not appropriate in every case. Your ophthalmologist and anesthesiologist will decide if it is right for your child and for the surgery being performed.
Can a parent be with the child while anesthesia is given?
Each hospital will have its own policies about parents being with the child during the time the child is going to sleep in the operating room or waking up in the recovery room. Ask your doctor about specific policies at your hospital.
What happens during the recovery from general anesthesia after surgery?
Once the surgery is complete, the anesthesiologist will begin to wake up the patient. This may take several minutes or longer. Once it is safe to do so, the tube is removed and normal breathing resumes. The child is then transferred from the operating room to the recovery room and over the next hour or so will continue to gradually wake up.. During this time children are often groggy, irritable and confused. They will receive constant supportive care and reassurance from the recovery room staff, who are also monitoring the child’s heart rate, blood pressure, pain level and breathing. During the next few hours the child will still be sleepy, sometimes cranky, and may have a lowered tolerance for discomfort or pain. Additional reassurance and the use of mild pain medications are helpful when needed. Most children are back to many normal activities by the next day. Occasionally a child will sleep for hours after a procedure, especially after a long surgery or if sedating pain medications are required.
What are the side effects of anesthesia?
Children may be nauseated or vomit after eye surgery, particularly muscle surgery. Although the nausea may last for hours, it is rarely serious. Everything possible should be done to reassure the child and make him or her comfortable. Medication is sometimes helpful.
What are the risks of anesthesia?
Serious anesthesia complications, such as brain damage or death, are exceptionally rare. Generally healthy children tolerate anesthesia at least as well as adults.
Whenever possible, elective eye surgery should be avoided when the child is ill. Anesthesiologists and surgeons should be informed of all medical conditions and all medications the child is taking. They should also be informed of any anesthetic problems the child or any blood relative has experienced, as there are some rare hereditary conditions, which are associated with a greater risk.
Some studies have shown that children under 4 years of age who receive anesthesia may be at an increased risk of long term neurodevelopmental effects and/or learning disabilities. This is currently an active area of research as physicians and scientists work to learn more about how to most safely provide anesthesia to the youngest patients. These risks may be outweighed by the benefits of a medically necessary procedure. When a surgery is needed to improve a child’s development, it is not advisable to delay it until after four years of age. Talk with your child’s physician prior to surgery about the risks and benefits of surgery or an examination which requires general anesthesia. You can also read this for further information: http://www.pedsanesthesia.org/Consensus_Statement_Dec_2012.pdf(this statement is current)
Although eye surgery is usually quite routine, children are extensively monitored by the anesthesiologist while they are asleep. Serious reactions to anesthesia are extremely rare. All precautions are taken to ensure children’s safety while they are asleep. Please discuss all your questions with your child’s anesthesiologist prior to surgery.
Can strabismus surgery in pediatric patients be done with topical or local anesthesia?
Generally, no. Rarely, in a select group of exceptionally stoic teenagers and adults, strabismus surgery can be done with a local anesthetic injection through the lower eyelid to numb the nerves around the eyeball. Unlike its use in adult cataract surgery, topical anesthesia, consisting of numbing eye drops to the surface of the eye, does not provide sufficient patient comfort to be used during eye muscle surgery. Strabismus surgery typically requires 30 minutes and often significantly longer. The patient must be completely still and comfortable during this period to avoid potentially serious complications that may result from sudden unexpected movements. As most children cannot be expected to remain still for the time necessary to complete the surgery, nearly all children require general anesthesia in order for eye muscle surgery to be performed safely and comfortably.
Summary
Anesthesia for children is generally safe. Complications may be minimized by avoiding food and drink before general anesthesia and postponing elective surgery if the child is ill. Modern anesthesia allows surgery or examinations to be performed without pain or anxiety.
Credits: Journal of American Association for Pediatric Ophthalmology and Strabismus